The BAOMS Annual Conference 2015 was held in Liverpool at the ACC under the presidency of Professor James Brown, one of my colleagues from the maxillofacial surgery department at University Hospital Aintree. It was a great meeting and I gave a keynote lecture entitled “The challenges of rehabilitation following maxillary & mid-face malignancy”.
I covered the main challenges of treating rare tumours (less than 6% of head and neck cancers) in this critical anatomical site and went through the classification popularised by James Brown as a guide to decision making..Treatments including free flap reconstruction and prosthetic obturation were discussed together with indications for the insertion of zygomatic and co-axis dental implants at the time of surgery in order to optimise the prosthetic obturation of the resulting defect.
By inserting implants at the time of surgery, we can proceed to early loading of these fixtures with bar supported obturators which have in-built support and retention within the defect where it is required. This provides a much more stable and retentive device for the patient to use, removes the need for the use of soft degradable lining materials to engage the sensitive cavity, making the device much lower profile and easier to insert and maintain. Hard acrylic materials which can be highly polished provide durable and cleanable restorations which don’t result in nasal blockage or deterioration.
For low level Brown Class I defects the option to close the maxillary sinus exposure with a buccal advancement flap together with the buccal fat pad together with the insertion of implants allows the production of a precision fixed or removable implant retained prosthesis while eliminating a maxillary defect with its inherent disadvantages.
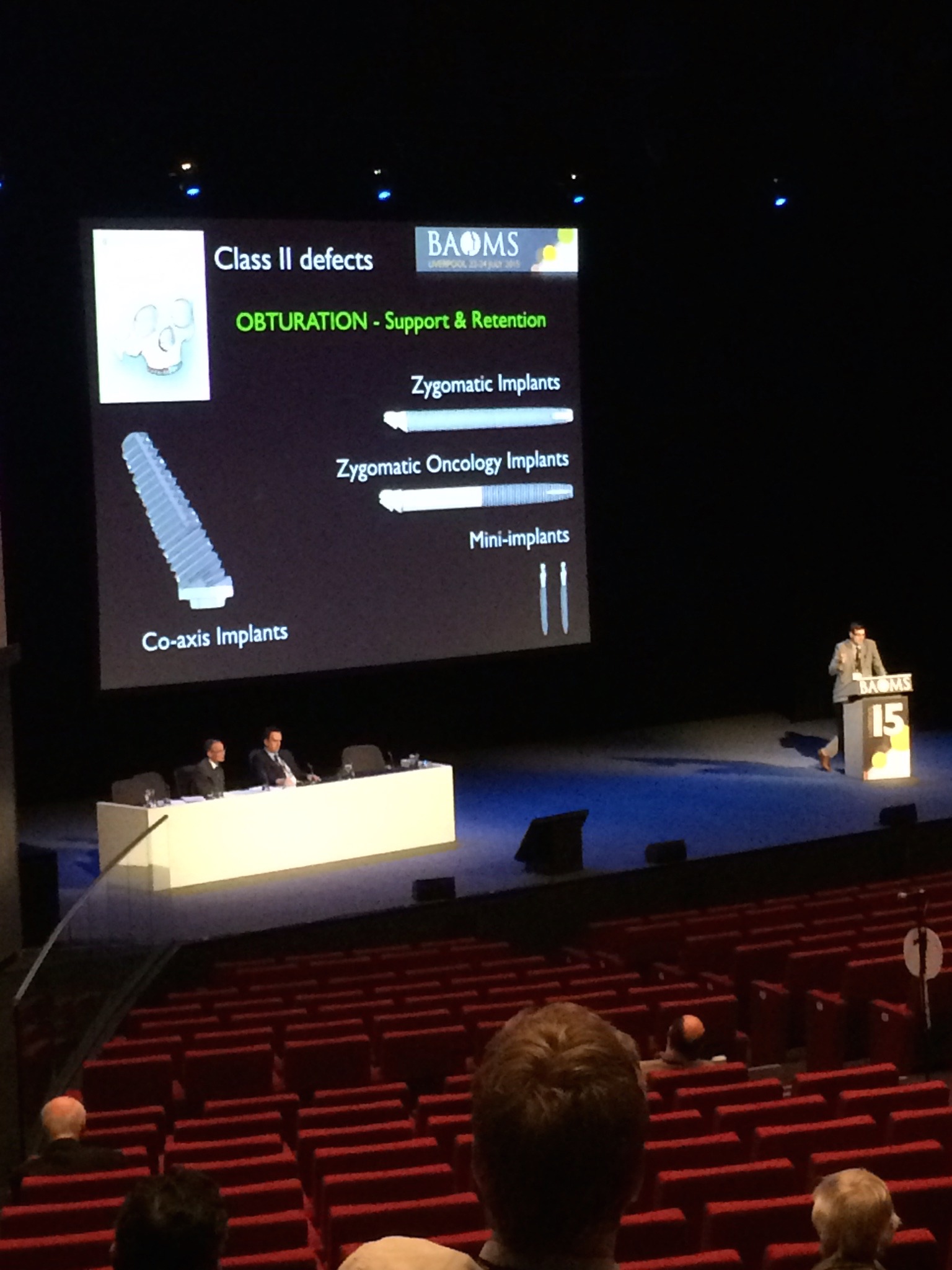
In class II defects, there are options to obturate or use free vascularised tissue depending on various patient factors and clinician opportunities. The use of soft tissue free flaps should be restricted to the posterior maxilla (distal to the canine) if a true rehabilitative approach is being taken. For defects with a larger horizontal component, composite free flaps (DCIA or fibula) should be employed as a suitable foundation for later dental rehabilitation on implants.
Where obturation is the approach only small posterior defects should be treated without implants and restored with simple dental retained obturators. Once the canine tooth is involved in a unilateral defect or where the defect is larger or where the remaining dentition is missing or of poor prognosis, immediate implants should be inserted.
I presented my large series (n=38 pts, 103 zygomatic implants) of zygomatic implants used in oncology patients. Interestingly the primary and secondary placement groups contain the same number of inserted zygomatic implants currently (n=51 implants per group).
The survival rate for the primary placement group was 94% and the secondary group was 88% giving an indication that there is no better time to place zygomatic implants in oncology patients than at the time of initial operation.
This lecture is now available on the Members-only part of this website – to view please apply for membership..
[Best_Wordpress_Gallery id=”4″ gal_title=”BAOMS 2015″]